Activity Based Funding
In last year’s newsletter, we explained the benefits of assigning an ICD 10 code to each patient attendance at an ED or Injury Unit and the important role that it plays in assigning an Urgency Related Grouper, for the purposes of Activity Based Funding, to each attendance. This will mean that, for the first time, the ED phase of care will receive specific funding, in contrast to the current situation where block funding does not recognise individual ED attendances and the ED phase of care prior to admission, for those patients admitted to an inpatient bed, is not funded separately.
The diagram shows the five data points required for each patient attendance to allow that attendance be allocated to 1 of 114 Urgency Related Groupers (URGs). The URG, in combination with a parallel exercise in patient level costing for each hospital, is the means by which funding is allocated for each patient attendance.
The first four pieces of data are already returned from each hospital to the Business Information Unit as part of the PET return. If any of the five pieces of data is missing, the attendance will be assigned to an error URG, which means the unit will only receive a fraction of the funding for the attendance that it would have received had all five pieces of data been returned.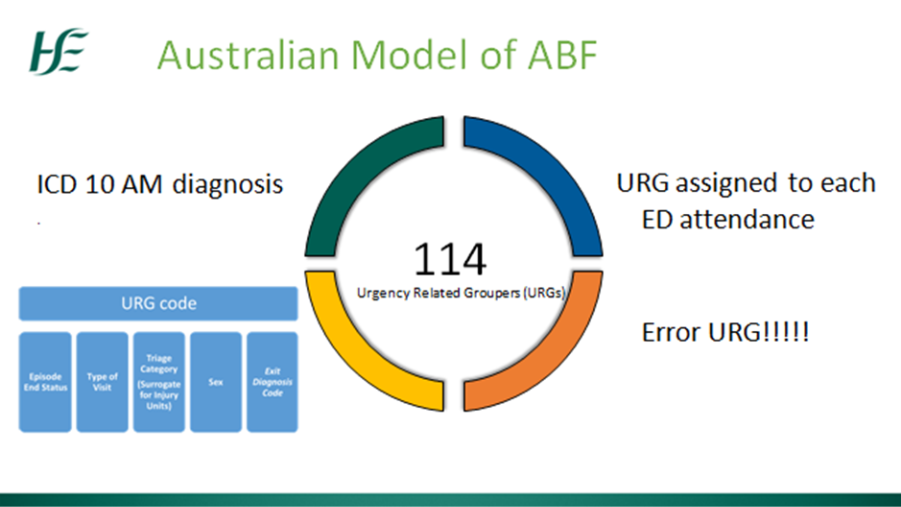
Every ED and Injury Unit has now been visited at least once and various means of facilitating the progression of this project have been employed outside of direct visits.
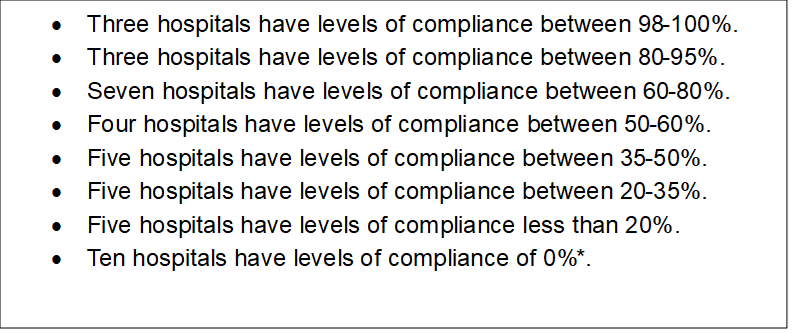
In terms of percentage compliance with coding of all attendances at EDs and Injury Units the following is the situation as of week ending 16th December:
*Almost all of the hospitals with a compliance level of 0% are upgrading or changing IT systems and have definite plans to commence coding in the near future.
The Healthcare Pricing Office is currently collecting and analysing the data as it is returned, to allow as comprehensive an analysis of activity as is possible. This will allow a URG to be assigned to each attendance with a diagnosis code, before proceeding to incorporate the URG with patient level costing for each hospital, with a view to proceeding to a period of shadow ABF funding, where each hospital will see the funding they would receive after the move from block funding to ABF.
|